Frequently
Asked Questions
|
- What is Childhood Asthma?
If he has a persistent cough that is accompanied by noisy breathing/wheezing or rapid breathing, he is diagnosed or suspected of having childhood asthma. If the symptoms are recurrent, occurring once or twice a month or for more than two months, there may be a family history of allergies or asthma in the parents or other siblings, and the kid may have childhood or early-onset asthma. - Is it true that every youngster who coughs develops Asthma?
Many children have a cough that is accompanied by a runny nose, a blocked nose, sinusitis, or snoring. Coughing can be particularly bothersome at night or while lying down. He might not have trouble breathing or wheezing. Still, the child suffers from cough-type asthma. This can be studied further by doing a Lung Function Test, which aids in the diagnosis of asthma. Imaging of the sinuses or adenoids may be required for the child. It can be addressed with the right medications. - Is it true that all children with asthma have trouble breathing or have a loud chest?
No, a child with asthma may just have a dry or moist cough, and they may need to increase their exercise and physical activity, such as dancing or running. He or she may have a clear cheat, which means there are no sounds coming from the chest. To diagnose asthma in such children, a skilled Pediatric Pulmonologist should perform a lung function test. - What does a Lung Function Test entail?
This is a sophisticated, internationally recognised test in which a child or any patient exhales inhaled air rapidly and deeply into a mouthpiece attached to a device. This gauge measures the amount of air evacuated from the lungs in one second or the total volume of air expelled over three or six seconds. It’s a kid-friendly test that includes rewards such as blowing candles or balloons. A competent Pediatric Pulmonologist can do this procedure on a child as young as three to four years old. It detects the true obstruction in a child’s small airways in the chest. - Is childhood asthma a chronic illness or a taboo?
No, Asthma in children can begin as early as 1-2 years of age. It might become more severe if the symptoms persist and there is a family history of allergies or asthma. It can be completely managed and treated with correct diagnosis and therapy. The medications or puffs are provided for a sufficient amount of time with no negative side effects. This problem is under control and is unlikely to recur. - Is it possible for my child to be harmed by medications such as an inhaler or a puff?
No, There are no side effects or long-term growth difficulties if inhalers or puffs are prescribed by a physician following a thorough examination and administered through spacer with good technique. In comparison to steroids administered by nebulizers, inhaled steroids administered via spacer are measured in micrograms (mg). As a result, there are no significant adverse effects. - What should I do if my child has a noisy breathing pattern or a continuous X-ray patch?
Contact a paediatric pulmonologist if your child is under the age of two years old and has noisy breathing, feeding difficulties/sleep problems, is not growing well, or is vomiting at night or after a meal. It’s possible that the youngster has a congenital issue, such as malacia or GERD. He may need a Bronchoscop to view his airways to determine his problem, or he may need medication. - Is a young child infected with tuberculosis?
If your kid has a chronic fever, cough, isn’t eating well, is losing or gaining weight, or has persistent chest shadows, see your doctor. If there is a history of contact with anybody who has TB, go to the doctor right away. Few tests are performed, and in a small kid, a bronchoscopy may be required to evaluate a sputum specimen. Tuberculosis can be totally treated with the right testing and medications. - What is gastroesophageal reflux disease (GERD)?
Symptoms of GERD in children can vary. He may experience early morning nausea or vomiting, gagging, aversion to milk or liquids, abdominal pain, nocturnal cough/coughs after feeds, and a lack of weight gain. It has the potential to aggravate asthma symptoms. It can be treated with the right medications and a healthy diet. - What is Allergy?
Allergy is characterized by a heightened sensitivity to allergens inhaled through the air or consumed through sensitive food products. Coughing, running nose, nasal itching, red or watery eyes, breathing problems, wheezing, or skin itching/rash are all symptoms. - What exactly are allergens, and how do they influence our bodies?
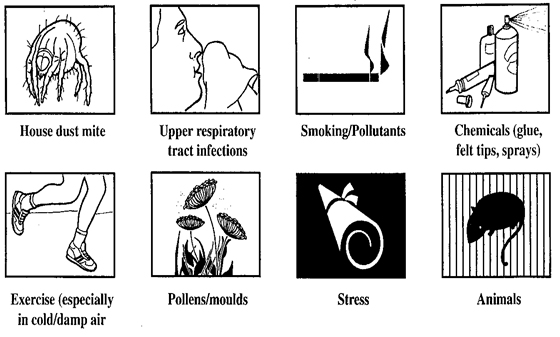
Airborne allergens such as house dust mites, pollens, insects, rice dust, wheat dust, house dust, fungal spores, and food allergens such as nuts, baker yeast, lentils, egg/milk/non-veg., etc. can cause allergic reactions. Coughing, nasal congestion, skin rash, itching, breathing difficulties, and sputum production are all common symptoms. This can happen at any time of year, not only at the changing of seasons.
- What is Bronchitis/Asthma, and how does it affect you?
Bronchitis is a condition in which the main branches of the lungs, the Bronchi, enlarge. In children, it can induce recurrent coughing, post-cough vomiting, and breathing difficulties. It could be only momentary or last for a long period.

- Is it true that children who have Asthma will always have Asthma?
Asthma isn’t a taboo subject. Childhood asthma is caused by the enlargement of small bronchial tubes, which can prevent air from passing and easily allow mucus to clog the tubes. If there is no history of asthma or allergies in the family, most youngsters can be completely controlled with adequate medication.